
For all health plans, quality is a constant imperative. But CMS Star Ratings add incentives to the mission that allow plans to expand their clinical reach and elevate the level of care delivered to every member, despite any obstacles they may encounter.
In 2023, when the Centers for Medicare & Medicaid Services (CMS) introduced the Medicare Advantage and Part D Final Rule, the agency sent a clear message: Your overall Star Rating is closely linked to how well you serve members with social risk factors (SRFs). Whether you are navigating the complexities of the original Health Equity Index framework or the newly proposed EHO4all shifts, generic member engagement is no longer a viable strategy.
Now, health plans must look beyond automated calls and printed mailers. They must embrace pharmacist-led care powered by advanced pharmacy technology to close persistent healthcare disparities and protect their performance.
What is health equity?
Health equity is the state in which every individual has a fair and just opportunity to attain their highest level of health. Achieving this requires more than equal access to care; it requires identifying and removing systemic obstacles, such as income, geographic location, and language barriers, that lead to healthcare disparities. As noted by the World Health Organization, “Health equity is achieved when everyone can attain their full potential for health and well-being.”
Imagine a health plan member whose primary language isn’t English, but receives a medication regimen entirely in English. For this person, it would be difficult to understand the instructions for their medication since they’re not outlined in a way that’s useful for them. This leads to the patient not taking their medication as prescribed, which could increase the likelihood of hospital readmission. But, when looking at this patient through a lens that’s focused on health equity, access barriers are removed by identifying language as a challenge and ensuring the patient receives translated instructions.
While the industry has long discussed closing care gaps, the CMS Health Equity Index (HEI) has turned these discussions into a performance-based reality.
What is the CMS health equity index (HEI)?
You may hear the HEI referred to as the Excellent Health Outcomes for All (EHO4all) reward. CMS recently introduced this name to better reflect the goal: ensuring that high-quality, pharmacist-led care reaches every member, regardless of their socioeconomic status. Despite the name change, the goals remain the same.
The HEI (EHO4all Reward) is the latest in CMS’s commitment to driving improved health outcomes in socially vulnerable communities. This reward is a performance-based scoring tool designed to incentivize Medicare Advantage (MA) and Part D plans to improve care for members who face significant healthcare disparities.
CMS considers members who fall into the categories below as socially vulnerable and will include them in the measures:
- Members receiving a low-income subsidy
- Members who are dually eligible for Medicare and Medicaid
- Members with a disability (those with a disability and/or end-stage renal disease as the original reason for entitlement to Medicare under age 65).
While these factors remain intact for the latest 2027 Star Ratings, CMS may add additional factors in the future, including those based on geographic location.
 How to calculate the CMS Health Equity Index
How to calculate the CMS Health Equity Index

The HEI calculation is a three-step process that evaluates how well your plan serves members with social risk factors, specifically those who are dual eligible, receive a low-income subsidy, or are disabled.
1. The tertile performance score
CMS looks at a subset of your existing CMS quality measures, like HEDIS and CAHPS. For each of these measures, CMS compares your performance only for members with SRFs against the performance of all other plans for that same subgroup.
Plans are then ranked and divided into tertiles (thirds):
- Top third: +1 point
- Middle third: 0 points
- Bottom third: -1 point
2. Calculating the HEI score
Once each of your relevant CMS quality measures has been assigned a point (-1, 0, or 1) based on how you performed compared to other plans, it’s time to find your average.
Think of this like a GPA for health equity. CMS looks at all the points you earned across different measures, like medication adherence for diabetes or blood pressure control, and calculates a weighted average. This calculation gives you a final HEI score that lands somewhere between -1 and +1. If your score is 0 or lower, you aren't eligible for a reward.
3. Reward factor
The final step determines how much the HEI Score actually increases your overall CMS Star Ratings. This is where the size of your at-risk population matters. CMS looks at the percentage of your members who have social risk factors and compares that to the national average.
- Low concentration: If your plan has very few at-risk members (well below the national average), you won’t receive an HEI reward, even if your score is high.
- Medium concentration: If your at-risk population is around the national average, you can earn additional points. Your HEI score is multiplied by 0.2 and added to your Star Rating.
- High concentration: If you serve a higher-than-average percentage of at-risk members, you are eligible for a larger sum of additional points. Your HEI Score is multiplied by 0.4 and added to your Star Rating.

Why the HEI is the new financial engine for star ratings
In the Medicare Advantage world, Star Ratings are the ultimate lever for financial survival. A plan’s rating determines two major things: whether it receives a Quality Bonus Payment based on rating and how much of an incentive it can gain to offer better benefits to members.
Why does this matter for health plans? For a high-performing plan with many at-risk members, this HEI reward can result in a 0.4-star increase. In a world where a half-star can mean millions of dollars in quality bonus payments, this calculation is the difference between a 3.5-star plan and a 4-star plan. It’s worth noting that reaching 4 stars has the potential to unlock millions of dollars in additional revenue that can be reinvested into the plan.
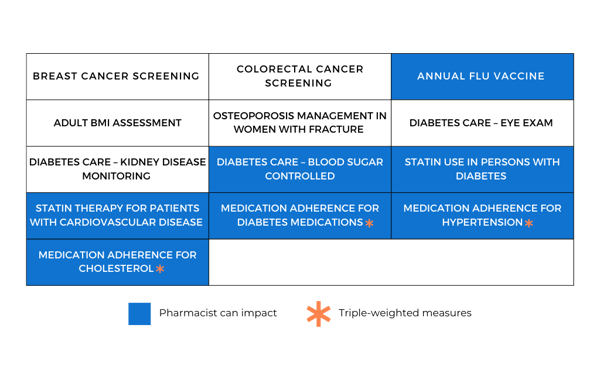
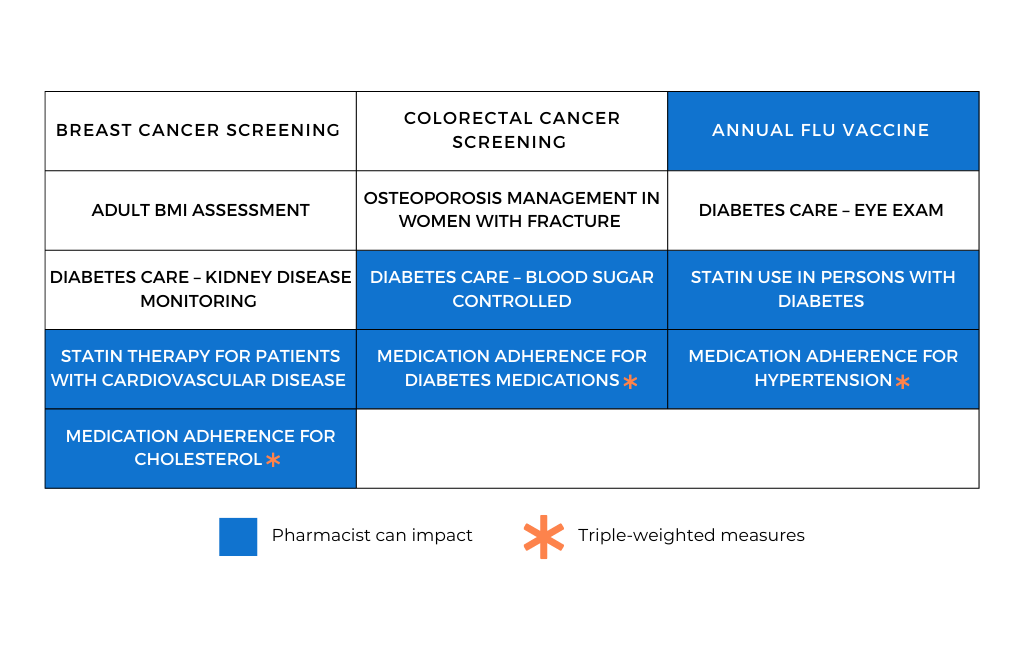
CMS is now putting the money where the need is: rewarding plans that prove they can close gaps for members facing the most significant obstacles. Because medication adherence measures are triple-weighted (meaning they count three times as much as other measures), they are the fastest way to improve your HEI score.
By using pharmacy technology to provide pharmacist-led care specifically for eligible members, you aren't just doing the right thing to help your member population; you're making a smart financial move. It ensures your plan stays in the top tier, secures that 0.4-star boost, and protects your financial future.
Pharmacy technology as a health equity equalizer
Not only does equitable access to pharmacy care help improve outcomes, but it’s also a massive opportunity to rethink how you engage your most vulnerable members. You don't have to navigate these changes with outdated, manual processes that fail to reach the people who need help the most.
The good news is that outsourced pharmacy services make a direct impact on the most highly weighted HEI measures. That’s because pharmacists can empower members to take a more active role in their health and reach them through digital channels rather than requiring them to drive to a pharmacy or clinic. There are nearly countless ways for pharmacists to improve health outcomes for the most socially at-risk members. These include boosting medication adherence, educating about the benefits of routine vaccinations, or counseling on medication interactions.
No matter if you have in-house pharmacists and need an end-to-end technology solution, or you’re looking to tap into the power of Aspen RxHealth’s nationwide network of remote pharmacists, we’re ready and able to help serve health plans just like yours.
Reach out to us today to learn more about the Health Equity Index and speak with a member of our team.
